

Description
Psoriatic arthritis is a condition involving joint inflammation (arthritis) that usually occurs in combination with a skin disorder called psoriasis. Psoriasis is a chronic inflammatory condition characterized by patches of red, irritated skin that are often covered by flaky white scales. People with psoriasis may also have changes in their fingernails and toenails, such as nails that become pitted or ridged, crumble, or separate from the nail beds.
Signs and symptoms of psoriatic arthritis include stiff, painful joints with redness, heat, and swelling in the surrounding tissues. When the hands and feet are affected, swelling and redness may result in a "sausage-like" appearance of the fingers or toes (dactylitis).
In most people with psoriatic arthritis, psoriasis appears before joint problems develop. Psoriasis typically begins during adolescence or young adulthood, and psoriatic arthritis usually occurs between the ages of 30 and 50. However, both conditions may occur at any age. In a small number of cases, psoriatic arthritis develops in the absence of noticeable skin changes.
Psoriatic arthritis may be difficult to distinguish from other forms of arthritis, particularly when skin changes are minimal or absent. Nail changes and dactylitis are two features that are characteristic of psoriatic arthritis, although they do not occur in all cases.
Psoriatic arthritis is categorized into five types: distal interphalangeal predominant, asymmetric oligoarticular, symmetric polyarthritis, spondylitis, and arthritis mutilans.
The distal interphalangeal predominant type affects mainly the ends of the fingers and toes. The distal interphalangeal joints are those closest to the nails. Nail changes are especially frequent with this form of psoriatic arthritis.
The asymmetric oligoarticular and symmetric polyarthritis types are the most common forms of psoriatic arthritis. The asymmetric oligoarticular type of psoriatic arthritis involves different joints on each side of the body, while the symmetric polyarthritis form affects the same joints on each side. Any joint in the body may be affected in these forms of the disorder, and symptoms range from mild to severe.
Some individuals with psoriatic arthritis have joint involvement that primarily involves spondylitis, which is inflammation in the joints between the vertebrae in the spine. Symptoms of this form of the disorder involve pain and stiffness in the back or neck, and movement is often impaired. Joints in the arms, legs, hands, and feet may also be involved.
The most severe and least common type of psoriatic arthritis is called arthritis mutilans. Fewer than 5 percent of individuals with psoriatic arthritis have this form of the disorder. Arthritis mutilans involves severe inflammation that damages the joints in the hands and feet, resulting in deformation and movement problems. Bone loss (osteolysis) at the joints may lead to shortening (telescoping) of the fingers and toes. Neck and back pain may also occur.
Frequency
Psoriatic arthritis affects an estimated 24 in 10,000 people.
Between 5 and 10 percent of people with psoriasis develop psoriatic arthritis, according to most estimates. Some studies suggest a figure as high as 30 percent. Psoriasis itself is a common disorder, affecting approximately 2 to 3 percent of the population worldwide.
Causes
The specific cause of psoriatic arthritis is unknown. Its signs and symptoms result from excessive inflammation in and around the joints. Inflammation occurs when the immune system sends signaling molecules and white blood cells to a site of injury or disease to fight microbial invaders and facilitate tissue repair. When this has been accomplished, the body ordinarily stops the inflammatory response to prevent damage to its own cells and tissues. Mechanical stress on the joints, such as occurs in movement, may result in an excessive inflammatory response in people with psoriatic arthritis. The reasons for this excessive inflammatory response are unclear.
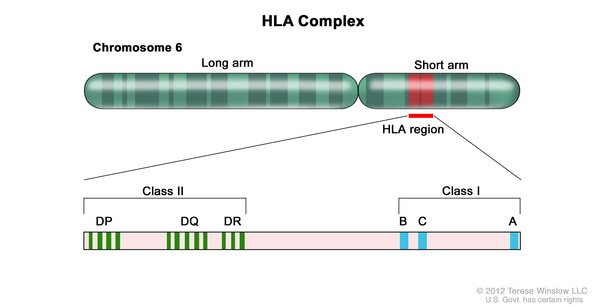
Researchers have identified changes in several genes that may influence the risk of developing psoriatic arthritis. The most well-studied of these genes belong to a family of genes called the human leukocyte antigen (HLA) complex. The HLA complex helps the immune system distinguish the body's own proteins from proteins made by foreign invaders (such as viruses and bacteria). Each HLA gene has many different normal variations, allowing each person's immune system to react to a wide range of foreign proteins. Variations of several HLA genes seem to affect the risk of developing psoriatic arthritis, as well as the type, severity, and progression of the condition.
Variations in several other genes have also been associated with psoriatic arthritis. Many of these genes are thought to play roles in immune system function. However, variations in these genes probably make only a small contribution to the overall risk of developing psoriatic arthritis. Other genetic and environmental factors are also likely to influence a person's chances of developing this disorder.
Inheritance
This condition has an unknown inheritance pattern. Approximately 40 percent of affected individuals have at least one close family member with psoriasis or psoriatic arthritis.
Other Names for This Condition
- Arthropathic psoriasis
- Psoriatic arthropathy
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Castelino M, Barton A. Genetic susceptibility factors for psoriatic arthritis. Curr Opin Rheumatol. 2010 Mar;22(2):152-6. doi: 10.1097/BOR.0b013e32833669d2. Citation on PubMed
- Chandran V, Raychaudhuri SP. Geoepidemiology and environmental factors of psoriasis and psoriatic arthritis. J Autoimmun. 2010 May;34(3):J314-21. doi: 10.1016/j.jaut.2009.12.001. Epub 2009 Dec 24. Citation on PubMed
- Gladman DD. Psoriatic arthritis. Dermatol Ther. 2009 Jan-Feb;22(1):40-55. doi: 10.1111/j.1529-8019.2008.01215.x. Citation on PubMed
- Jordan CT, Cao L, Roberson ED, Pierson KC, Yang CF, Joyce CE, Ryan C, Duan S, Helms CA, Liu Y, Chen Y, McBride AA, Hwu WL, Wu JY, Chen YT, Menter A, Goldbach-Mansky R, Lowes MA, Bowcock AM. PSORS2 is due to mutations in CARD14. Am J Hum Genet. 2012 May 4;90(5):784-95. doi: 10.1016/j.ajhg.2012.03.012. Epub 2012 Apr 19. Citation on PubMed or Free article on PubMed Central
- McGonagle D, Benjamin M, Tan AL. The pathogenesis of psoriatic arthritis and associated nail disease: not autoimmune after all? Curr Opin Rheumatol. 2009 Jul;21(4):340-7. doi: 10.1097/BOR.0b013e32832c6ab9. Citation on PubMed
- McGonagle D, Palmou Fontana N, Tan AL, Benjamin M. Nailing down the genetic and immunological basis for psoriatic disease. Dermatology. 2010;221 Suppl 1:15-22. doi: 10.1159/000316171. Epub 2010 Aug 9. Citation on PubMed
- Nograles KE, Brasington RD, Bowcock AM. New insights into the pathogenesis and genetics of psoriatic arthritis. Nat Clin Pract Rheumatol. 2009 Feb;5(2):83-91. doi: 10.1038/ncprheum0987. Citation on PubMed or Free article on PubMed Central
- O'Rielly DD, Rahman P. Where do we stand with the genetics of psoriatic arthritis? Curr Rheumatol Rep. 2010 Aug;12(4):300-8. doi: 10.1007/s11926-010-0111-4. Citation on PubMed
- Ritchlin C. Psoriatic disease--from skin to bone. Nat Clin Pract Rheumatol. 2007 Dec;3(12):698-706. doi: 10.1038/ncprheum0670. Citation on PubMed
- Wollina U, Unger L, Heinig B, Kittner T. Psoriatic arthritis. Dermatol Ther. 2010 Mar-Apr;23(2):123-36. doi: 10.1111/j.1529-8019.2010.01306.x. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.