

Description
Non-alcoholic fatty liver disease (NAFLD) is a buildup of excessive fat in the liver that can lead to liver damage resembling the damage caused by alcohol abuse, but that occurs in people who do not drink heavily. The liver is a part of the digestive system that helps break down food, store energy, and remove waste products, including toxins. The liver normally contains some fat; an individual is considered to have a fatty liver (hepatic steatosis) if the liver contains more than 5 to 10 percent fat.
The fat deposits in the liver associated with NAFLD usually cause no symptoms, although they may cause increased levels of liver enzymes that are detected in routine blood tests. Some affected individuals have abdominal pain or fatigue. During a physical examination, the liver may be found to be slightly enlarged.
Between 7 and 30 percent of people with NAFLD develop inflammation of the liver (non-alcoholic steatohepatitis, also known as NASH), leading to liver damage. Minor damage to the liver can be repaired by the body. However, severe or long-term damage can lead to the replacement of normal liver tissue with scar tissue (fibrosis), resulting in irreversible liver disease (cirrhosis) that causes the liver to stop working properly. Signs and symptoms of cirrhosis, which get worse as fibrosis affects more of the liver, include fatigue, weakness, loss of appetite, weight loss, nausea, swelling (edema), and yellowing of the skin and whites of the eyes (jaundice). Scarring in the vein that carries blood into the liver from the other digestive organs (the portal vein) can lead to increased pressure in that blood vessel (portal hypertension), resulting in swollen blood vessels (varices) within the digestive system. Rupture of these varices can cause life-threatening bleeding.
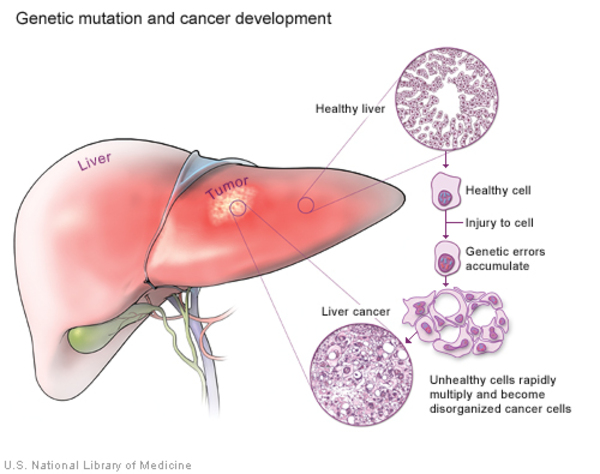
NAFLD and NASH are thought to account for many cases of cirrhosis that have no obvious underlying cause (cryptogenic cirrhosis); at least one-third of people with NASH eventually develop cirrhosis. People with NAFLD, NASH, and cirrhosis are also at increased risk of developing liver cancer (hepatocellular cancer).
NAFLD is most common in middle-aged or older people, although younger people, including children, are also affected. It is often considered as part of a group of conditions known collectively as the metabolic syndrome; in addition to NAFLD, the metabolic syndrome includes obesity, type 2 diabetes or pre-diabetes (insulin resistance), high levels of fats (lipids) such as cholesterol and triglycerides in the blood, and high blood pressure (hypertension). However, a person with NAFLD may not have all or any of the other conditions that make up the metabolic syndrome, and individuals with some or all of those conditions may not have NAFLD.
Frequency
NAFLD is a very common disorder, occurring in about 25 percent of the global population. Its prevalence is increasing along with the rising prevalence of obesity in industrialized societies, and it is now the most common chronic liver disorder in Western countries, including the United States. NAFLD is more prevalent in individuals of Hispanic, Native American, or Asian ancestry than in individuals of European or African ancestry.
Causes
The specific causes of NAFLD are unclear. Genetic variations and environmental factors contribute to the development of this complex disorder.
When fat from the diet exceeds the body's requirements and ability to break it down and eliminate it, some of the fat is stored in the liver. Researchers suggest that over-consumption of certain specific nutrients, such as iron, cholesterol, and refined sugars used in processed foods, may increase the likelihood of developing NAFLD.
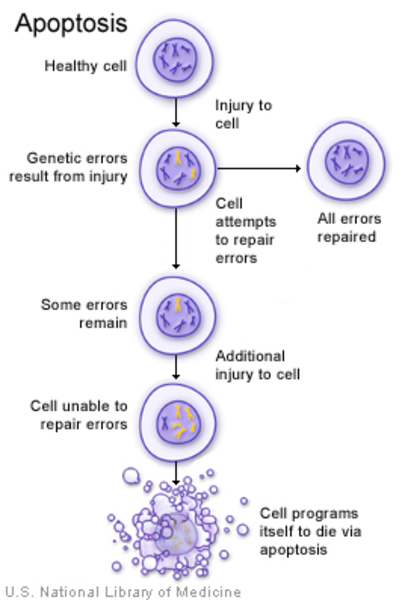
It is unclear what causes NASH and cirrhosis to develop in some people with NAFLD. Researchers are studying several possible mechanisms. These include inflammation caused by an immune system reaction to the excess fatty tissue in the liver; toxic inflammatory chemicals (cytokines) released by the liver cells or fat cells; self-destruction (apoptosis) of liver cells; and the effect of unstable molecules called free radicals (oxidative stress). The effects of different populations of microorganisms in the intestines (gut microbiota) on the breakdown and absorption of nutrients are also an active area of research.
Studies have identified many genetic changes that may be associated with the development of NAFLD and NASH. Among these is a particular variation in the PNPLA3 gene. This gene provides instructions for making a protein called adiponutrin, which is found in fat cells (adipocytes) and liver cells (hepatocytes). The function of this protein is not well understood, but it is thought to help regulate the production and breakdown of fats (lipogenesis and lipolysis) and the development of adipocytes. Studies indicate that the activity (expression) of the PNPLA3 gene decreases during periods without food (fasting) and increases after eating, suggesting that the amount of adiponutrin protein produced is regulated as needed to help process and store fats in the diet. The PNPLA3 gene variation associated with NAFLD is thought to lead to increased production and decreased breakdown of fats in the liver. Research is ongoing to determine how this and other genetic changes contribute to the development of NAFLD and its complications.
Inheritance
An increased risk of developing NAFLD can be passed through generations in families, but the inheritance pattern is unknown. Variations in several genes as well as lifestyle and environmental factors contribute to the risk of developing this complex disorder.
Other Names for This Condition
- Fatty liver
- NAFLD
- NASH
- Non-alcoholic steatohepatitis
- Nonalcoholic fatty liver disease
- Nonalcoholic steatohepatitis
- Steatosis
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Caligiuri A, Gentilini A, Marra F. Molecular Pathogenesis of NASH. Int J Mol Sci. 2016 Sep 20;17(9):1575. doi: 10.3390/ijms17091575. Citation on PubMed or Free article on PubMed Central
- Chen LZ, Xin YN, Geng N, Jiang M, Zhang DD, Xuan SY. PNPLA3 I148M variant in nonalcoholic fatty liver disease: demographic and ethnic characteristics and the role of the variant in nonalcoholic fatty liver fibrosis. World J Gastroenterol. 2015 Jan 21;21(3):794-802. doi: 10.3748/wjg.v21.i3.794. Citation on PubMed or Free article on PubMed Central
- Dongiovanni P, Donati B, Fares R, Lombardi R, Mancina RM, Romeo S, Valenti L. PNPLA3 I148M polymorphism and progressive liver disease. World J Gastroenterol. 2013 Nov 7;19(41):6969-78. doi: 10.3748/wjg.v19.i41.6969. Citation on PubMed or Free article on PubMed Central
- Gu J, Yao M, Yao D, Wang L, Yang X, Yao D. Nonalcoholic Lipid Accumulation and Hepatocyte Malignant Transformation. J Clin Transl Hepatol. 2016 Jun 28;4(2):123-30. doi: 10.14218/JCTH.2016.00010. Epub 2016 Jun 15. Citation on PubMed or Free article on PubMed Central
- Kahali B, Halligan B, Speliotes EK. Insights from Genome-Wide Association Analyses of Nonalcoholic Fatty Liver Disease. Semin Liver Dis. 2015 Nov;35(4):375-91. doi: 10.1055/s-0035-1567870. Epub 2015 Dec 16. Citation on PubMed or Free article on PubMed Central
- Kitamoto A, Kitamoto T, Nakamura T, Ogawa Y, Yoneda M, Hyogo H, Ochi H, Mizusawa S, Ueno T, Nakao K, Sekine A, Chayama K, Nakajima A, Hotta K. Association of polymorphisms in GCKR and TRIB1 with nonalcoholic fatty liver disease and metabolic syndrome traits. Endocr J. 2014;61(7):683-9. doi: 10.1507/endocrj.ej14-0052. Epub 2014 May 1. Citation on PubMed
- Krawczyk M, Portincasa P, Lammert F. PNPLA3-associated steatohepatitis: toward a gene-based classification of fatty liver disease. Semin Liver Dis. 2013 Nov;33(4):369-79. doi: 10.1055/s-0033-1358525. Epub 2013 Nov 12. Citation on PubMed
- Mancina RM, Dongiovanni P, Petta S, Pingitore P, Meroni M, Rametta R, Boren J, Montalcini T, Pujia A, Wiklund O, Hindy G, Spagnuolo R, Motta BM, Pipitone RM, Craxi A, Fargion S, Nobili V, Kakela P, Karja V, Mannisto V, Pihlajamaki J, Reilly DF, Castro-Perez J, Kozlitina J, Valenti L, Romeo S. The MBOAT7-TMC4 Variant rs641738 Increases Risk of Nonalcoholic Fatty Liver Disease in Individuals of European Descent. Gastroenterology. 2016 May;150(5):1219-1230.e6. doi: 10.1053/j.gastro.2016.01.032. Epub 2016 Feb 2. Citation on PubMed or Free article on PubMed Central
- Severson TJ, Besur S, Bonkovsky HL. Genetic factors that affect nonalcoholic fatty liver disease: A systematic clinical review. World J Gastroenterol. 2016 Aug 7;22(29):6742-56. doi: 10.3748/wjg.v22.i29.6742. Citation on PubMed or Free article on PubMed Central
- Yu J, Marsh S, Hu J, Feng W, Wu C. The Pathogenesis of Nonalcoholic Fatty Liver Disease: Interplay between Diet, Gut Microbiota, and Genetic Background. Gastroenterol Res Pract. 2016;2016:2862173. doi: 10.1155/2016/2862173. Epub 2016 May 9. Citation on PubMed or Free article on PubMed Central
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.