

Description
Immune thrombocytopenia is a disorder characterized by a blood abnormality called thrombocytopenia, which is a shortage of blood cells called platelets that are needed for normal blood clotting.
Affected individuals can develop red or purple spots on the skin caused by bleeding just under the skin's surface. Small spots of bleeding under the skin are called purpura and larger spots are called ecchymoses. People with immune thrombocytopenia can have significant bleeding episodes, such as nose bleeds (epistaxis) or bleeding in the moist lining (mucosae) of the mouth. In severe cases, individuals may have gastrointestinal bleeding or blood in the urine or stool, or heavy and prolonged menstrual bleeding (menorrhagia). In very rare instances, bleeding inside the skull (intracranial hemorrhage) can occur, which can be life-threatening. A greater reduction in platelet numbers is often associated with more frequent bleeding episodes and an increased risk of severe bleeding.
While immune thrombocytopenia can be diagnosed at any age, there are two periods when the condition is most likely to develop: early childhood and late adulthood. In children, the reduction in platelets is often sudden, but platelet levels usually return to normal levels within weeks to months. Immune thrombocytopenia in children is often preceded by a minor infection, such as an upper respiratory infection, but the relationship between the infection and immune thrombocytopenia is not clear. In adults, the development of immune thrombocytopenia is usually gradual and the condition tends to persist throughout life.
Frequency
The incidence of immune thrombocytopenia is approximately 4 per 100,000 children and 3 per 100,000 adults. In adults with immune thrombocytopenia, women are affected more often than men.
It is likely that this condition is underdiagnosed because those with mild signs and symptoms often do not seek medical attention.
Causes
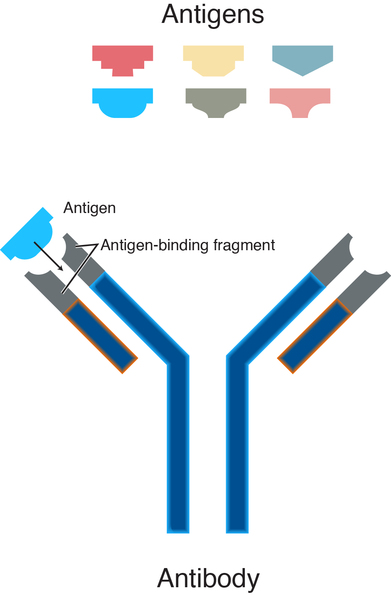
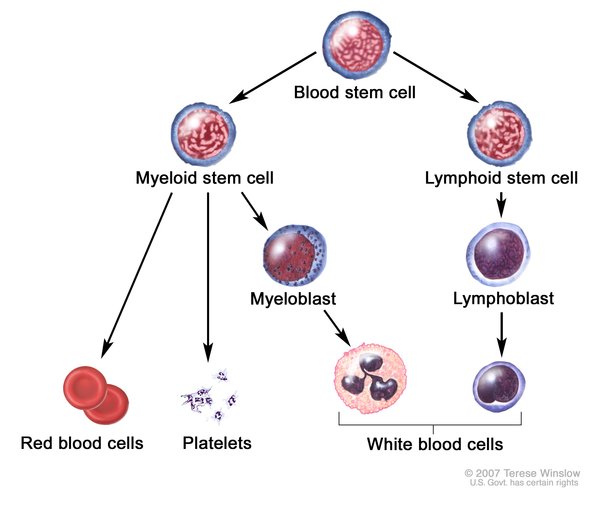
The genetic cause of immune thrombocytopenia is unclear. This condition occurs when the body's own immune system malfunctions and attacks the body's tissues and organs (autoimmunity). Normally, the immune system produces proteins called antibodies, which attach to specific foreign particles and germs, marking them for destruction. In immune thrombocytopenia, the immune system abnormally destroys platelets and makes fewer platelets than normal. People with immune thrombocytopenia produce antibodies that attack normal platelets. The platelets are destroyed and eliminated from the body, resulting in a shortage of these cells in affected individuals. Some of these antibodies also affect the cells in the bone marrow that produce platelets (known as megakaryocytes), which leads to a decrease in platelet production, further reducing the number of platelets in the blood.

In some people with immune thrombocytopenia, the abnormal immune reactions may coincide with an infection by certain viruses or bacteria. Exposure to these foreign invaders may trigger the body to fight the infection, but the immune system also mistakenly attacks platelets.
Genetic variations (polymorphisms) in a few genes have been found in some people with immune thrombocytopenia and may increase the risk of abnormal immune reactions. However, the contribution of these genetic changes to the development of immune thrombocytopenia is unclear.
When the condition is due to the targeted destruction of platelets by the body's own immune cells, it is known as primary immune thrombocytopenia. Immune thrombocytopenia following bacterial or viral infection is considered primary because the infection triggers a platelet-specific immune reaction, typically without any other signs or symptoms. However, immune thrombocytopenia can be a feature of other immune disorders, such as common variable immune deficiency, which occurs when the immune system has a decreased ability to protect the body against foreign invaders, or other autoimmune disorders such as systemic lupus erythematosus. Immune thrombocytopenia can also occur with other blood disorders, including a form of cancer of the blood-forming tissue known as chronic lymphocytic leukemia, and human immunodeficiency virus (HIV) infection. When immune thrombocytopenia is a feature of other disorders, the condition is known as secondary immune thrombocytopenia.
Inheritance
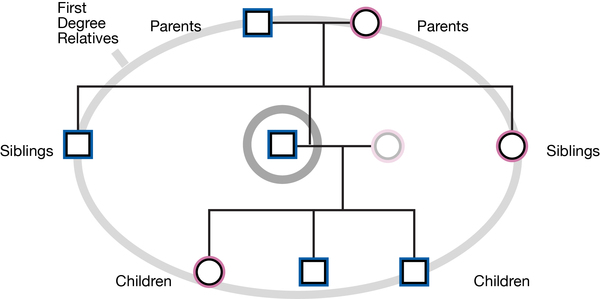
Immune thrombocytopenia and other autoimmune disorders can run in families, but the inheritance pattern is usually unknown. People with a first-degree relative (such as a parent or sibling) with immune thrombocytopenia likely have an increased risk of developing the disorder themselves.
Other Names for This Condition
- Autoimmune thrombocytopenia
- Autoimmune thrombocytopenic purpura
- Idiopathic thrombocytopenic purpura
- Immune thrombocytopenic purpura
- ITP
- Werlhof disease
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Alam MM. Idiopathic thrombocytopenic purpura in children: a 10 years experience at tertiary care hospital. J Pak Med Assoc. 2014 Dec;64(12):1358-62. Citation on PubMed
- Arnold DM. Bleeding complications in immune thrombocytopenia. Hematology Am Soc Hematol Educ Program. 2015;2015:237-42. doi: 10.1182/asheducation-2015.1.237. Citation on PubMed
- Doobaree IU, Nandigam R, Bennett D, Newland A, Provan D. Thromboembolism in adults with primary immune thrombocytopenia: a systematic literature review and meta-analysis. Eur J Haematol. 2016 Oct;97(4):321-30. doi: 10.1111/ejh.12777. Epub 2016 Jun 20. Citation on PubMed
- Neunert C, Noroozi N, Norman G, Buchanan GR, Goy J, Nazi I, Kelton JG, Arnold DM. Severe bleeding events in adults and children with primary immune thrombocytopenia: a systematic review. J Thromb Haemost. 2015 Mar;13(3):457-64. doi: 10.1111/jth.12813. Epub 2015 Jan 14. Citation on PubMed
- Ozkan MC, Sahin F, Saydam G. Immune thrombocytopenic purpura: new biological therapy of an old disease. Curr Med Chem. 2015;22(16):1956-62. doi: 10.2174/0929867322666150319102830. Citation on PubMed
- Provan D, Newland AC. Current Management of Primary Immune Thrombocytopenia. Adv Ther. 2015 Oct;32(10):875-87. doi: 10.1007/s12325-015-0251-z. Epub 2015 Oct 26. Citation on PubMed or Free article on PubMed Central
- Provan D, Stasi R, Newland AC, Blanchette VS, Bolton-Maggs P, Bussel JB, Chong BH, Cines DB, Gernsheimer TB, Godeau B, Grainger J, Greer I, Hunt BJ, Imbach PA, Lyons G, McMillan R, Rodeghiero F, Sanz MA, Tarantino M, Watson S, Young J, Kuter DJ. International consensus report on the investigation and management of primary immune thrombocytopenia. Blood. 2010 Jan 14;115(2):168-86. doi: 10.1182/blood-2009-06-225565. Epub 2009 Oct 21. Citation on PubMed
- Rodeghiero F, Stasi R, Gernsheimer T, Michel M, Provan D, Arnold DM, Bussel JB, Cines DB, Chong BH, Cooper N, Godeau B, Lechner K, Mazzucconi MG, McMillan R, Sanz MA, Imbach P, Blanchette V, Kuhne T, Ruggeri M, George JN. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009 Mar 12;113(11):2386-93. doi: 10.1182/blood-2008-07-162503. Epub 2008 Nov 12. Citation on PubMed
- Smalisz-Skrzypczyk K, Romiszewski M, Matysiak M, Demkow U, Pawelec K. The Influence of Primary Cytomegalovirus or Epstein-Barr Virus Infection on the Course of Idiopathic Thrombocytopenic Purpura. Adv Exp Med Biol. 2016;878:83-8. doi: 10.1007/5584_2015_162. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.