






Cytochrome P450 oxidoreductase deficiency is a disorder of hormone production. This condition specifically affects steroid hormones, which are needed for normal development and reproduction. The hormonal changes associated with cytochrome P450 oxidoreductase deficiency can affect the development of the reproductive system, skeleton, and other parts of the body. These signs and symptoms are usually present at birth or become apparent in early childhood.
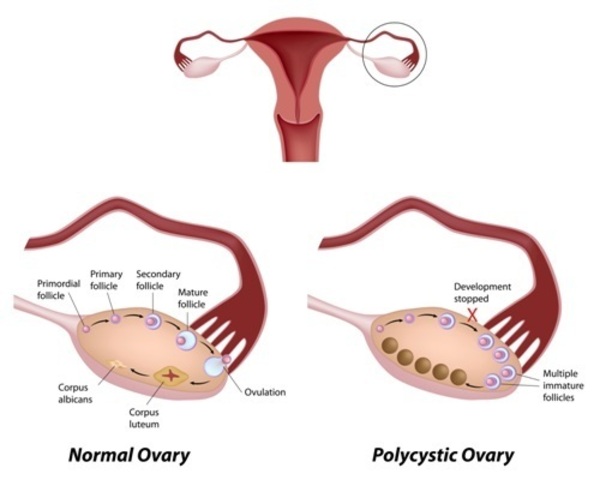
The signs and symptoms of cytochrome P450 oxidoreductase deficiency vary from mild to severe. Signs and symptoms of mild cases can include a failure to begin menstruation by age 16 (primary amenorrhea), an inability to have biological children (infertility) in both men and women, and a condition called polycystic ovarian syndrome (PCOS). PCOS is characterized by a hormonal imbalance in women that can lead to irregular menstruation, acne, excess body hair (hirsutism), and weight gain.
People with moderate cases of cytochrome P450 oxidoreductase deficiency may have external genitalia that do not look clearly male or female, and they may have infertility. People with moderate cytochrome P450 oxidoreductase deficiency usually do not have skeletal abnormalities.
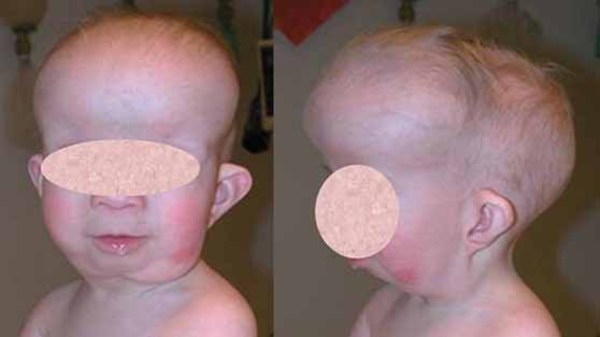
The severe form of cytochrome P450 oxidoreductase deficiency is sometimes called Antley-Bixler syndrome with genital anomalies and disordered steroidogenesis. Hormonal changes in affected males and females lead to the development of genital differences, as well as infertility. Severe cases are also characterized by skeletal abnormalities, particularly involving bones of the head and face. These include premature fusion of the skull bones (craniosynostosis), a flattened mid-face, a prominent forehead, and low-set ears. Other skeletal abnormalities can include joint deformities (contractures) that limit movement; unusually long, slender fingers (arachnodactyly); bowing of the thigh bones; and radiohumeral synostosis, which is a bone abnormality that locks the elbows in a bent position. A blockage of the nasal passages (choanal atresia), intellectual disability, and delayed development are also associated with the severe form of the disorder.

Some women who are pregnant with fetuses affected by cytochrome P450 oxidoreductase deficiency experience mild symptoms of the disorder even though they themselves do not have the disorder. They may develop excessive body hair growth (hirsutism), acne, and a deep voice. These changes go away soon after delivery.
Frequency
The prevalence of cytochrome P450 oxidoreductase deficiency is unknown. About 65 cases have been reported worldwide.
Researchers suspect that cytochrome P450 oxidoreductase deficiency is underdiagnosed and that mild cases of this disorder may be relatively common. Because the signs and symptoms can be difficult to detect, people with mild cytochrome P450 oxidoreductase deficiency may never come to medical attention.
Causes
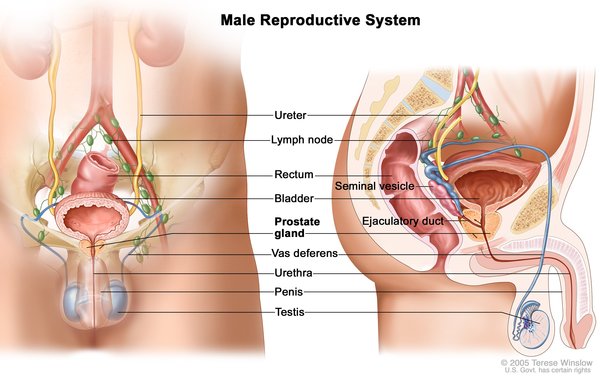
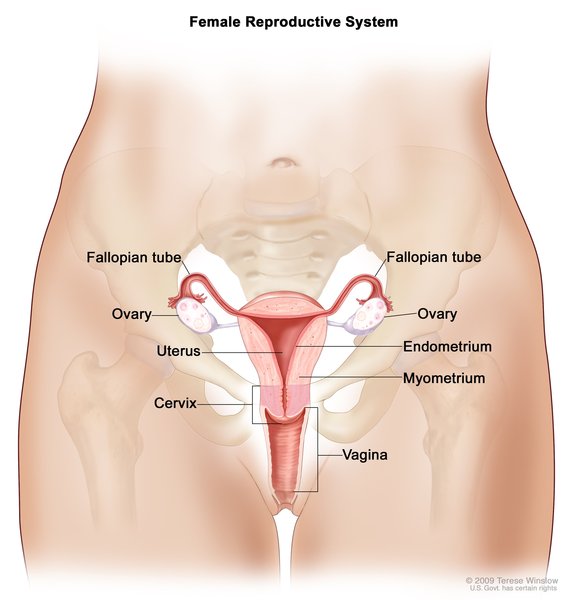
Cytochrome P450 oxidoreductase deficiency is caused by mutations in the POR gene. This gene provides instructions for making the enzyme cytochrome P450 oxidoreductase, which plays a critical role in the formation of steroid hormones. This group of hormones includes testosterone and estrogen, which are essential for normal sexual development and reproduction; corticosteroids, which are involved in the body's response to stress; and aldosterone, which helps regulate the body's salt and water balance.
Mutations in the POR gene reduce the activity of cytochrome P450 oxidoreductase, which disrupts the production of steroid hormones. Changes in sex hormones such as testosterone and estrogen lead to problems with sexual development before birth and at puberty. In a woman who is pregnant with an affected fetus, abnormal levels of sex hormones in the fetus may cause her to have mild, temporary signs and symptoms of cytochrome P450 oxidoreductase deficiency.
Cytochrome P450 oxidoreductase is also needed for the production of cholesterol. This substance has many essential functions both before and after birth, including roles in the production of steroid hormones and in the formation and growth of bones. Mutations in the POR gene can disrupt the production of cholesterol, which likely impairs normal bone formation in the severe form of cytochrome P450 oxidoreductase deficiency. Studies suggest that a molecule called retinoic acid also plays a role in the skeletal abnormalities found in severe cases. The breakdown of retinoic acid requires cytochrome P450 oxidoreductase; if a shortage of cytochrome P450 oxidoreductase prevents retinoic acid from being broken down, the resulting excess of that molecule can stimulate the abnormal growth and fusion of bones.
The skeletal abnormalities found in the severe form of this disorder can also result from mutations in another gene, FGFR2. Some researchers use the name Antley-Bixler syndrome to describe these features, whether they are caused by mutations in the POR gene or in the FGFR2 gene. Others use the name Antley-Bixler syndrome with genital anomalies and disordered steroidogenesis for cases caused by POR gene mutations, reserving the name Antley-Bixler syndrome for cases caused by FGFR2 gene mutations.
Inheritance
This condition is inherited in an autosomal recessive pattern, which means both copies of the gene in each cell have mutations. The parents of an individual with an autosomal recessive condition each carry one copy of the mutated gene, but they typically do not show signs and symptoms of the condition.

Other Names for This Condition
- Antley-Bixler syndrome
- Antley-Bixler syndrome with disordered steroidogenesis
- Antley-Bixler syndrome-like phenotype with disordered steroidogenesis
- Combined partial deficiency of 17-hydroxylase and 21-hydroxylase
- Congenital adrenal hyperplasia due to apparent combined p450c17 and p450c21 deficiency
- POR deficiency
- PORD
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Arlt W. P450 oxidoreductase deficiency and Antley-Bixler syndrome. Rev Endocr Metab Disord. 2007 Dec;8(4):301-7. doi: 10.1007/s11154-007-9056-y. Citation on PubMed
- Fluck CE, Pandey AV. Clinical and biochemical consequences of p450 oxidoreductase deficiency. Endocr Dev. 2011;20:63-79. doi: 10.1159/000321221. Epub 2010 Dec 16. Citation on PubMed
- Fluck CE, Tajima T, Pandey AV, Arlt W, Okuhara K, Verge CF, Jabs EW, Mendonca BB, Fujieda K, Miller WL. Mutant P450 oxidoreductase causes disordered steroidogenesis with and without Antley-Bixler syndrome. Nat Genet. 2004 Mar;36(3):228-30. doi: 10.1038/ng1300. Epub 2004 Feb 1. Citation on PubMed
- Fukami M, Horikawa R, Nagai T, Tanaka T, Naiki Y, Sato N, Okuyama T, Nakai H, Soneda S, Tachibana K, Matsuo N, Sato S, Homma K, Nishimura G, Hasegawa T, Ogata T. Cytochrome P450 oxidoreductase gene mutations and Antley-Bixler syndrome with abnormal genitalia and/or impaired steroidogenesis: molecular and clinical studies in 10 patients. J Clin Endocrinol Metab. 2005 Jan;90(1):414-26. doi: 10.1210/jc.2004-0810. Epub 2004 Oct 13. Citation on PubMed
- Huang N, Pandey AV, Agrawal V, Reardon W, Lapunzina PD, Mowat D, Jabs EW, Van Vliet G, Sack J, Fluck CE, Miller WL. Diversity and function of mutations in p450 oxidoreductase in patients with Antley-Bixler syndrome and disordered steroidogenesis. Am J Hum Genet. 2005 May;76(5):729-49. doi: 10.1086/429417. Epub 2005 Mar 25. Citation on PubMed or Free article on PubMed Central
- Miller WL, Huang N, Pandey AV, Fluck CE, Agrawal V. P450 oxidoreductase deficiency: a new disorder of steroidogenesis. Ann N Y Acad Sci. 2005 Dec;1061:100-8. doi: 10.1196/annals.1336.012. Citation on PubMed
- Miller WL. P450 oxidoreductase deficiency: a disorder of steroidogenesis with multiple clinical manifestations. Sci Signal. 2012 Oct 23;5(247):pt11. doi: 10.1126/scisignal.2003318. Citation on PubMed
- Porter FD, Herman GE. Malformation syndromes caused by disorders of cholesterol synthesis. J Lipid Res. 2011 Jan;52(1):6-34. doi: 10.1194/jlr.R009548. Epub 2010 Oct 7. Citation on PubMed or Free article on PubMed Central
- Sahakitrungruang T, Huang N, Tee MK, Agrawal V, Russell WE, Crock P, Murphy N, Migeon CJ, Miller WL. Clinical, genetic, and enzymatic characterization of P450 oxidoreductase deficiency in four patients. J Clin Endocrinol Metab. 2009 Dec;94(12):4992-5000. doi: 10.1210/jc.2009-1460. Epub 2009 Oct 16. Citation on PubMed or Free article on PubMed Central
- Scott RR, Miller WL. Genetic and clinical features of p450 oxidoreductase deficiency. Horm Res. 2008;69(5):266-75. doi: 10.1159/000114857. Epub 2008 Feb 6. Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.