

Description
Congenital central hypoventilation syndrome (CCHS) is a disorder that affects normal breathing. People with this disorder take shallow breaths (hypoventilate), especially during sleep, resulting in a shortage of oxygen and a buildup of carbon dioxide in the blood. Ordinarily, the part of the nervous system that controls involuntary body processes (autonomic nervous system) would react to such an imbalance by stimulating the individual to breathe more deeply or wake up. This nervous system reaction is impaired in people with CCHS. They must be supported with a machine to help them breathe (mechanical ventilation) or a device that stimulates a normal breathing pattern (diaphragm pacemaker). Some affected individuals need this support 24 hours a day, while others need it only at night.
Symptoms of CCHS usually become apparent shortly after birth when affected infants hypoventilate upon falling asleep. In these infants, a lack of oxygen in the blood often causes a bluish appearance of the skin or lips (cyanosis). In some milder cases, CCHS may not become apparent until later in life.
In addition to the breathing problem, people with CCHS may have difficulty regulating their heart rate and blood pressure, for example, in response to exercise or changes in body position. They also have decreased perception of pain, low body temperature, and occasional episodes of heavy sweating.
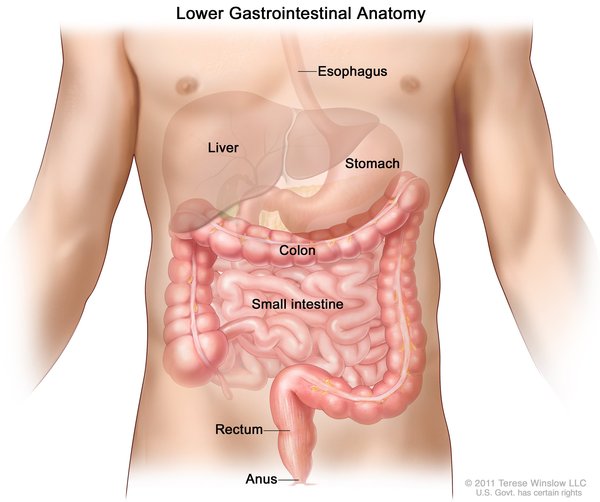
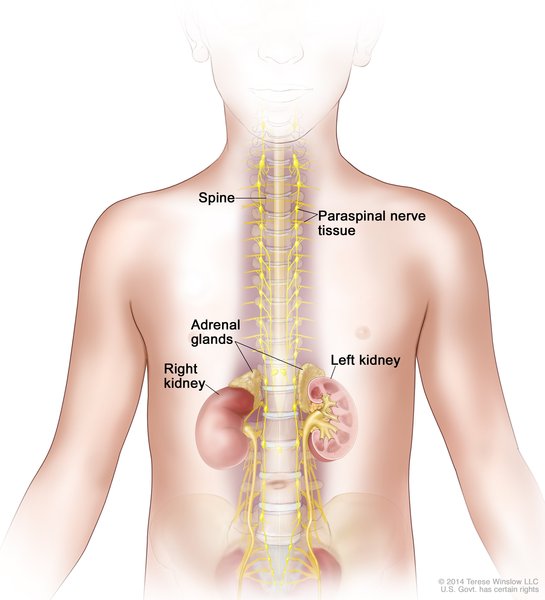
People with CCHS may have additional problems affecting the nervous system. About 20 percent of people with CCHS have abnormalities in the nerves that control the digestive tract (Hirschsprung disease), resulting in severe constipation, intestinal blockage, and enlargement of the colon. (Some researchers refer to the combination of CCHS and Hirschsprung disease as Haddad syndrome.) Some affected individuals develop learning difficulties or other neurological problems. People with CCHS are also at increased risk of developing certain tumors of the nervous system called neuroblastomas, ganglioneuromas, and ganglioneuroblastomas.
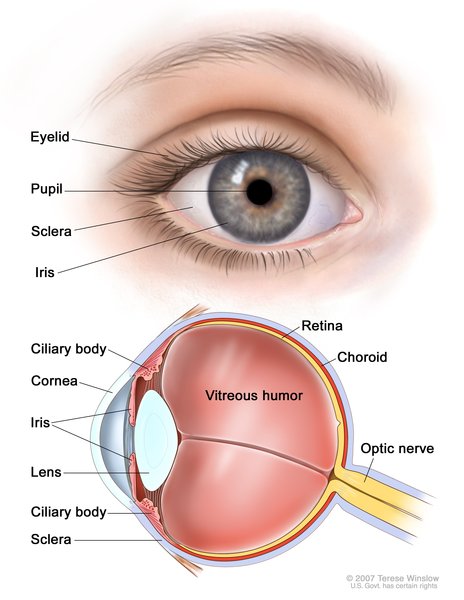
Additionally, individuals with CCHS usually have eye abnormalities, including a decreased response of the pupils to light. People with CCHS, especially children, may have a characteristic appearance with a short, wide, somewhat flattened face often described as "box-shaped."
In CCHS, life expectancy and the extent of any intellectual disabilities depend on the severity of the disorder, timing of the diagnosis, and the success of treatment.
Frequency
CCHS is a relatively rare disorder. More than 1,000 individuals with this condition have been identified. Researchers believe that some cases of sudden infant death syndrome (SIDS) or sudden unexplained death in children may be caused by undiagnosed CCHS.
Causes
Mutations in a gene called PHOX2B cause CCHS. The PHOX2B gene provides instructions for making a protein that is important during development before birth. The PHOX2B protein helps support the formation of nerve cells (neurons) and regulates the process by which the neurons mature to carry out specific functions (differentiation). The protein is active in the neural crest, which is a group of cells in the early embryo that give rise to many tissues and organs. Neural crest cells migrate to form parts of the autonomic nervous system, many tissues in the face and skull, and other tissue and cell types.

PHOX2B gene mutations that cause CCHS are believed to interfere with the PHOX2B protein's role in supporting neuron formation and differentiation, especially in the autonomic nervous system. As a result, bodily functions that are controlled by this system, including regulation of breathing, heart rate, blood pressure, and body temperature, are inconsistent in CCHS.
Inheritance
This condition is inherited in an autosomal dominant pattern, which means one copy of the altered gene in each cell is sufficient to cause the disorder.
More than 90 percent of cases of CCHS result from new mutations in the PHOX2B gene. These cases occur in people with no history of the disorder in their family. Occasionally an affected person inherits the mutation from one affected parent. The number of such cases has been increasing as better treatment has allowed more affected individuals to live into adulthood and start families.


About 5 to 10 percent of affected individuals inherit the altered gene from an unaffected parent who has a PHOX2B gene mutation only in their sperm or egg cells. This phenomenon is called germline mosaicism. A parent with mosaicism for a PHOX2B gene mutation may not show any signs or symptoms of CCHS.
Other Names for This Condition
- CCHS
- Congenital central hypoventilation
- Congenital failure of autonomic control
- Haddad syndrome
- Ondine syndrome
- Ondine-Hirschsprung disease
Additional Information & Resources
Genetic Testing Information
Genetic and Rare Diseases Information Center
Patient Support and Advocacy Resources
Clinical Trials
Catalog of Genes and Diseases from OMIM
Scientific Articles on PubMed
References
- Antic NA, Malow BA, Lange N, McEvoy RD, Olson AL, Turkington P, Windisch W, Samuels M, Stevens CA, Berry-Kravis EM, Weese-Mayer DE. PHOX2B mutation-confirmed congenital central hypoventilation syndrome: presentation in adulthood. Am J Respir Crit Care Med. 2006 Oct 15;174(8):923-7. doi: 10.1164/rccm.200605-607CR. Epub 2006 Jul 27. Citation on PubMed
- Berry-Kravis EM, Zhou L, Rand CM, Weese-Mayer DE. Congenital central hypoventilation syndrome: PHOX2B mutations and phenotype. Am J Respir Crit Care Med. 2006 Nov 15;174(10):1139-44. doi: 10.1164/rccm.200602-305OC. Epub 2006 Aug 3. Citation on PubMed
- Di Lascio S, Benfante R, Di Zanni E, Cardani S, Adamo A, Fornasari D, Ceccherini I, Bachetti T. Structural and functional differences in PHOX2B frameshift mutations underlie isolated or syndromic congenital central hypoventilation syndrome. Hum Mutat. 2018 Feb;39(2):219-236. doi: 10.1002/humu.23365. Epub 2017 Nov 21. Citation on PubMed or Free article on PubMed Central
- Kasi AS, Jurgensen TJ, Yen S, Kun SS, Keens TG, Perez IA. Three-Generation Family With Congenital Central Hypoventilation Syndrome and Novel PHOX2B Gene Non-Polyalanine Repeat Mutation. J Clin Sleep Med. 2017 Jul 15;13(7):925-927. doi: 10.5664/jcsm.6670. Citation on PubMed or Free article on PubMed Central
- Katwa U, D'Gama AM, Qualls AE, Donovan LM, Heffernan J, Shi J, Agrawal PB. Atypical presentations associated with non-polyalanine repeat PHOX2B mutations. Am J Med Genet A. 2018 Jul;176(7):1627-1631. doi: 10.1002/ajmg.a.38720. Epub 2018 Apr 28. Citation on PubMed or Free article on PubMed Central
- Paglietti MG, Cherchi C, Porcaro F, Agolini E, Schiavino A, Petreschi F, Novelli A, Cutrera R. Two novel mutations in exon 3 of PHOX2B gene: think about congenital central hypoventilation syndrome in patients with Hirschsprung disease. Ital J Pediatr. 2019 Apr 18;45(1):49. doi: 10.1186/s13052-019-0636-8. Citation on PubMed or Free article on PubMed Central
- Parodi S, Bachetti T, Lantieri F, Di Duca M, Santamaria G, Ottonello G, Matera I, Ravazzolo R, Ceccherini I. Parental origin and somatic mosaicism of PHOX2B mutations in Congenital Central Hypoventilation Syndrome. Hum Mutat. 2008 Jan;29(1):206. doi: 10.1002/humu.9516. Citation on PubMed
- Repetto GM, Corrales RJ, Abara SG, Zhou L, Berry-Kravis EM, Rand CM, Weese-Mayer DE. Later-onset congenital central hypoventilation syndrome due to a heterozygous 24-polyalanine repeat expansion mutation in the PHOX2B gene. Acta Paediatr. 2009 Jan;98(1):192-5. doi: 10.1111/j.1651-2227.2008.01039.x. Epub 2008 Sep 16. Citation on PubMed
- Sasaki A, Kishikawa Y, Imaji R, Fukushima Y, Nakamura Y, Nishimura Y, Yamada M, Mino Y, Mitsui T, Hayasaka K. Novel PHOX2B mutations in congenital central hypoventilation syndrome. Pediatr Int. 2019 Apr;61(4):393-396. doi: 10.1111/ped.13812. Epub 2019 Apr 17. Citation on PubMed
- Todd ES, Weinberg SM, Berry-Kravis EM, Silvestri JM, Kenny AS, Rand CM, Zhou L, Maher BS, Marazita ML, Weese-Mayer DE. Facial phenotype in children and young adults with PHOX2B-determined congenital central hypoventilation syndrome: quantitative pattern of dysmorphology. Pediatr Res. 2006 Jan;59(1):39-45. doi: 10.1203/01.pdr.0000191814.73340.1d. Epub 2005 Dec 2. Citation on PubMed
- Weese-Mayer DE, Berry-Kravis EM, Ceccherini I, Keens TG, Loghmanee DA, Trang H; ATS Congenital Central Hypoventilation Syndrome Subcommittee. An official ATS clinical policy statement: Congenital central hypoventilation syndrome: genetic basis, diagnosis, and management. Am J Respir Crit Care Med. 2010 Mar 15;181(6):626-44. doi: 10.1164/rccm.200807-1069ST. Citation on PubMed
- Weese-Mayer DE, Rand CM, Khaytin I, Slattery SM, Yap KL, Marazita ML, Berry-Kravis EM. Congenital Central Hypoventilation Syndrome. 2004 Jan 28 [updated 2021 Jan 28]. In: Adam MP, Feldman J, Mirzaa GM, Pagon RA, Wallace SE, Bean LJH, Gripp KW, Amemiya A, editors. GeneReviews(R) [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2024. Available from http://www.ncbi.nlm.nih.gov/books/NBK1427/ Citation on PubMed
The information on this site should not be used as a substitute for professional medical care or advice. Contact a health care provider if you have questions about your health.